Screening for Strabismus (Squint)
Strabismus or Squint is one of the most common eye problems encountered in children. It affects approximately 4% of children younger than 6 years and is an important cause of visual and psychological disablility.
Untreated, 30% to 50% will develop lazy eyes, or lose vision permanently, in the misaligned eye. Furthermore, proper ocular alignment is very necessary for normal development of binocular vision and depth perception.
 Causes of strabismus
Causes of strabismus
Strabismus can be either primary or secondary (acquired). Recognised risk factors for primary strabismus include a family history of strabismus, premature birth and a low birth weight. Secondary strabismus is often associated with neurological problems, such as intracranial tumours, head trauma, infection and autoimmune disorders
Types of strabismus
The most common type of strabismus involves horizontal misalignment of the eyes, although vertical misalignment also occurs. Squint may be manifest (tropia) or latent (phoria). Manifest ocular deviation can be present in all directions of gaze (comitant) or only present in specific directions of gaze (incomitant)
Screening tests for Strabismus
In the general practice setting, screening for strabismus involves four practical tests: the light reflex test, the red reflex test, the cover test and the uncover test. The only equipment required is a direct ophthalmoscope and a torchlight.
The light reflex test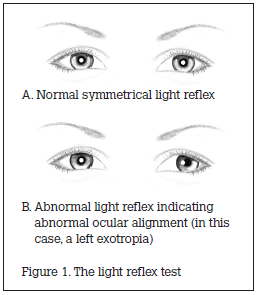
The child is placed on their parent’s lap. The doctor stands at a distance of 1 m in front of the child, holding a small light. The child’s attention is directed to the light. The position of the light’s reflection in each of the child’s eyes is noted and compared. Normal ocular alignment will generate an identical light reflection in each eye. Deflection of the light reflex indicates abnormal ocular alignment, with each 1 mm of deflection equivalent to 15–20 prism diopters deviation (Figure 1).

The red reflex test
The doctor stands at a distance of 0.5 m in front of the child, holding a direct ophthalmoscope (set at 0). The child’s attention is directed to the ophthalmoscope and the doctor attempts to visualise the red reflex of both eyes simultaneously. Both red reflexes should be identical. Inequality in size, shape or colour is abnormal (Figure 2).

The cover test
The doctor stands in front of the child and directs the child’s attention to a target (eg. a light or a toy). The doctor covers one of the child’s eyes and closely observes the uncovered eye for corrective movement. When the fixating normal eye is covered, a manifest abnormal eye must move from its deviated position and take up correct fixation. Accordingly, movement indicates that manifest strabismus is present in the uncovered eye (a tropia). The cover test is repeated on each eye (Figure 3).
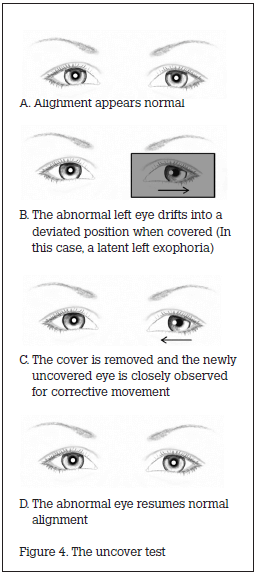
The uncover test
The doctor covers one of the child’s eyes for 5 seconds and directs the child’s attention to a target. The cover is then quickly removed. The newly uncovered eye is closely observed for corrective movement. A latent abnormal eye will drift into a deviated position when covered. After it is uncovered, the abnormal eye must then return to correct fixation. Accordingly, movement indicates that latent strabismus is present in the newly uncovered eye (a phoria). The uncover test is repeated on each eye (Figure 4).

Key Points for Practice |
| ● Patients with strabismus suffer functional and psychosocial problems related to their condition. |
| ● Early recognition and referral by Pediatricians is important as visual pathways may become permanently impaired if not addressed early. |
| ● All children with strabismus should be referred to a Pediatric Ophthalmologist for further assessment and visual rehabilitation. |
| ● The new onset of strabismus may be a red flag for serious intracranial or intraocular pathology. |
FAQs by parents of Children having Squint
Treatment of Squint in Children
Acknowledgment: RACGP guidelines for evaluating squint in children